Chargemaster maintenance is one of the most effective ways ambulatory surgery centers (ASCs) can maximize revenue, maintain compliance with contract terms, and strengthen payer negotiations. With claims denials and payment issues on the rise, even small deficiencies between charges and contracted rates can lead to significant underpayment.
ASCs can avoid revenue loss by conducting regular CPT-level and case-cost reviews, aligning charges with contractual allowances and future escalators, and addressing common gaps such as insufficient updates or inadequate pricing for bundled services.
A Hidden Revenue Loss Driver
Misaligned charges are one of the most overlooked drivers of revenue loss in ASCs. Even when contracts are favorable, poorly maintained chargemasters can effectively cap reimbursement and prevent ASCs from realizing the full value of their services.
At the center of this issue is the lesser-of provision, a standard contract clause that can significantly limit payment when charges are not properly aligned with allowed rates.
Most contracts reimburse based on the lesser of:
- 100% of billed charges.
- The contracted allowed amount per CPT.
If billed charges fall below the allowed amount, reimbursement is capped at the lower charge, resulting in lost revenue.
A key warning sign is when total payments (payer + patient responsibility) start to equal billed charges, indicating that charges may be set too low. Despite its simplicity, this remains one of the most common causes of contract revenue underperformance.
Below are four common scenarios ASCs encounter resulting in lost revenue due to lesser-of language.
Example One: Contract Escalators Outpace Charges
An ASC with contracts that include annual rate escalators finds that, by year three, payer-allowed amounts for high-volume procedures exceed 100% of billed charges, resulting in receipts equal to charges for those procedures.
Problem: Charges were not increased in line with contract escalators, resulting in payer-allowed amounts exceeding chargemaster levels, resulting in the provider being reimbursed at the lesser-of charge amount.
Takeaway: Annual chargemaster updates must exceed contractual escalators to maximize revenue for future years of payer contracts.
Example Two: Orthopedic Expansion without Charge Realignment
After adding orthopedic services, an ASC fails to adjust procedure charges to reflect high implant costs and diverse reimbursement structures.
Problem: Procedure charges did not account for payer methodologies that bundle implant reimbursement into procedure payments.
Table 1: Total Knee Scenario with Bundled Implant Reimbursement
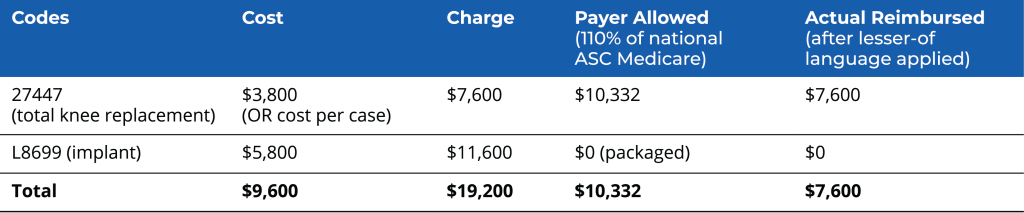
Lost Revenue = Actual Reimbursed – Payer Allowed ($7,600 – $10,332 = -$2,732)
Operating Cost Shortfall = Actual Reimbursed – Cost ($7,600 – $9,600 = -$2,000)
In this example, the ASC doubled the charge over the operating cost and implant cost for procedure code 27447 and the implant costs under HCPCS (L8699), resulting in an overall charge of $19,200. This is greater than the payer-allowed amount of $10,332, but the payer does not consider the implant charges when calculating the lesser of the billed charge for the case, as it bundles the implant reimbursement into the CPT codes.
When calculating reimbursement for the case, because implants are not reimbursed separately, the payer identifies whichever is lower: the allowed rate for procedure code 27447 or the billed charge amount for 27447. The total reimbursement for the case is $7,600, which is the billed charge for procedure code 27447. The payer reimbursed $2,732 below the allowed amount of $10,332 and $2,000 below the ASC’s operating cost for the case.
Takeaway: The charge for 27447 needs to be higher than the payer-allowed rate of $10,332 to capture the total reimbursement for this case.
Example Three: Charges Fail to Consider Payer’s Reimbursement Methodologies
The next illustration shows the impact of lesser-of language with bundled implant reimbursement and considers the payer reimbursement methodology for a rotator cuff repair case. The cost of this case, including implants, is $3,800, with total procedure charges (without implants) equal to $18,400.
Problem: Total costs may be covered by the actual reimbursed amount, but reimbursements are not maximized because the payer uses the billed charges to determine the lesser-of amounts.
Table 2: Rotator Cuff Repair (arthroscopic) with Biceps Tenodesis and Claviculectomy
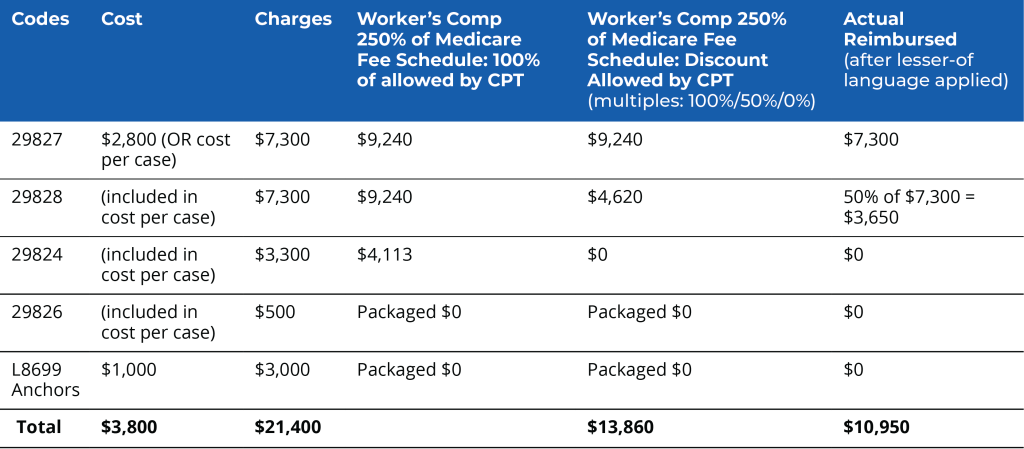
Lost Revenue = Actual Reimbursed – Payer Allowed ($10,950 – $13,860 = -$2,910)
Takeaway One: The charges for 29827, 29828, 29824, and 29826 must be higher than 100% of the payer-allowed amounts for each code to capture the maximum allowed reimbursement for this case.
Takeaway Two: When implants are bundled, or procedures in secondary and subsequent positions are discounted, procedure charges must be set high enough for the primary procedure code and for any additional procedure codes reimbursed in the case to account for total costs.
Example Four: Applying Multiple-Procedure Discounting to Charges
When reviewing billing data against a center’s chargemaster, we occasionally see billed charges that reflect a discounted amount (aligning with the payer’s policy on multiple-surgery discounts).
Problem: In these instances, the lesser-of logic is again applied by the payer, which further discounts the billed charges under its multiple-procedure policies.
Takeaway: ASCs should always bill their full charge for each code, including codes for procedures that are typically in the second- or subsequent-procedure position in a case.
Additional Chargemaster-Setting Considerations
While the lesser-of provision is a crucial factor in chargemaster performance, it does not operate in isolation. A well-optimized chargemaster requires ongoing attention to payer methodologies, contract limitations, and broader pricing strategy considerations.
1. Setting charges based on a percentage of Medicare rates is insufficient.
While Medicare benchmarks are useful for setting charges, they are not sufficient on their own. A more thorough approach includes
- Comparing charges to commercial payer fee schedules at the CPT level.
- Identifying CPTs where commercial rates exceed Medicare benchmarks.
- Performing a side-by-side CPT analysis to detect outliers.
It is also vital to account for future contract rates, including explicit rate increase and annual escalators or COLAs. This ensures chargemaster alignment throughout the life of a contract, not just the current year.
2. Pay attention to chargemaster limitation language.
Many payer contracts include provisions that restrict how and when chargemaster rates can be increased—often limiting updates to a defined percentage or a single annual adjustment. Because these limits can vary by payer, a compliant increase for one contract (e.g., tied to a COLA or escalator) may exceed what another payer allows, creating risk for reimbursement reductions.
Key considerations:
- Variation across contracts: Limits may differ by payer and may apply as flat caps or volume-weighted aggregate increases
- Ambiguity creates risk: Vague language can give payers discretion in interpreting compliance
- Negotiation opportunity: Where possible, remove or clarify limitations or secure higher caps
- Operational discipline: Track timing, notification requirements, and submission formats
- Pro tip: When reporting chargemaster increases to payers, include only payer-relevant CPTs and maintain documentation to support compliance
3. Usually, increases are contractually allowed only once in every 12-month period, so maintaining a consistent cadence is optimal.
Because many payer contracts limit the frequency of rate increases, timing is essential. Best practices:
- Review charges against contract rates on an annual basis.
- Reassess your chargemaster following new-payer rate and/or rate structure agreements.
- Ensure charges exceed all payer carve-out rates.
- Routine annual increases to stay ahead of negotiated rates.
Chargemaster maintenance is not merely an administrative exercise; it is a critical revenue-protection strategy. Regular, data-driven updates aligned with payer methodologies and contractual obligations ensure that ASCs fully capture the value of the care they deliver.
ECG’s ASC experts are happy to advise you on your chargemaster maintenance strategy.
Learn more about our work.

